You're busy. You don't have time to analyze the data, but you want to know if ACOs are working. This post is for you.
A couple months ago, J. Michael McWilliams published a summary of what we know about the Medicare Shared Savings Program (MSSP). The MSSP is the largest Medicare Accountable Care Organization (ACO) program, and McWilliams is a national expert on ACOs, having conducted and published numerous studies about them, a great deal of which I've written about on this blog or The Incidental Economist (see this, this, this, this, and this). So, how's the MSSP doing?
According to analysis by the Centers for Medicare and Medicaid Services (CMS) and a paper by McWilliams and colleagues, through 2013 the MSSP achieved "modest early spending reductions that were entirely offset by bonus payments." One reason bonuses outpaced savings is that 95% of MSSP ACOs faced no downside risk, meaning that CMS could not recoup costs from ACOs that spent above their benchmarks.
But, that's not the end of the story. In 2014, MSSP savings doubled and exceeded bonus payments by $287 million. (An analysis of MSSP savings from 2013 to 2014 by McWilliams is here.) This is, admittedly, a small fraction — 0.7% — of total spending on MSSP beneficiaries. However, McWilliams argues that this undercounts the savings because there are spillovers to non-MSSP beneficiaries. Additionally, because Medicare Advantage (MA) payments are now tied directly to traditional Medicare (TM) spending, any savings on the TM side reduces spending on the MA side. Accounting for these and other factors, McWilliams estimates that MSSP ACOs actually saved Medicare $685 million (1.6% of MSSP patient spending).
Though we tend to associate ACOs with Medicare, there are slightly more ACOs in the private than public sector. According to data from Leavitt Partners, fifty-four percent of ACOs are initiated by private insurers. What's new with those?
I wish I could tell you. Because they're initiated by many, different private insurers — whose data are, of course, closely held — there is no good way to comprehensively analyze private sector ACOs.
All is no lost. At least two private sector ACOs have been subjects of peer reviewed analysis: Blue Cross Blue Shield of Massachusetts Alternative Quality Contract — about which I've written — and, most recently, Cigna’s Collaborative Accountable Care (CAC) initiative — about which I have not (yet) written.
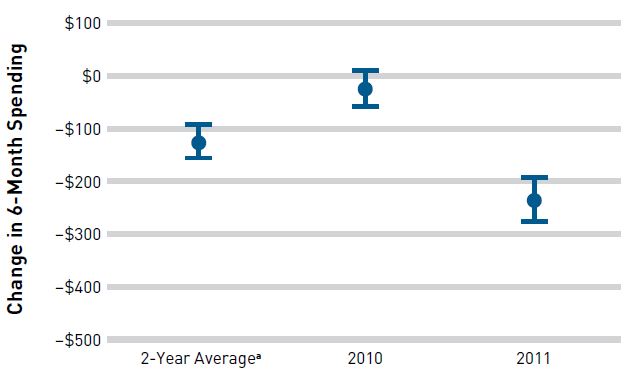
Last year, Vivian Ho and colleagues published analysis based on two years of the CAC initiative for the Medical Clinic of North Texas. It's a shared savings program that paid the clinic, in part, based on cost and quality. The clinic operated 42 practices with 141 primary care physicians serving over 7,000 patients. Using a propensity weighted difference-in-differences approach, the authors compared spending for clinic MCNT clinic patients to those visiting other PCPs in the same area between 2009 and 2011.
As shown in the chart below, no savings were detected in the first year, but the program did save money in the second. Over the two-year span, savings amounted to 5.7%, considerably larger than what has been achieved by the MSSP.
Yet, it may not be fair to compare the MSSP to the CAC/MCNT experience. The latter is just one private sector initiative, which may not generalize. In fact, the Blue Cross Blue Shield Alternative Quality contract saved about half as much as CAC/MCNT over two years.
Indeed, relatively modest savings are precisely what we should expect from a large, new program. McWilliams wrote,
Health care system reform is slow and incremental. Great strides are possible over a decade or two but require tradeoffs between short-term gains and long-term success. [...] It is time to acknowledge the early progress and allow policymakers to cast their gaze to the future.