By: Renee Gindi, Division of Health Interview Statistics
The National Center for Health Statistics (NCHS) is redesigning its well-respected household interview survey, the National Health Interview Survey (NHIS). The NHIS, the principal source of information on the nation’s health since 1957, is used by the public health research community to monitor trends in illness and disability, track progress toward achieving national health objectives, evaluate federal programs, and conduct epidemiologic and policy research. The survey will feature a new structure and updated content in 2018. This month, the first draft questionnaires were released to the public for comment.
Why Redesign?
Periodically the content of the NHIS is redesigned to ensure that the topics measured reflect the needs of the Department of Health and Human Services (HHS) and the public health community. The redesign aims to improve how relevant health topics are measured, and, as appropriate, to ensure that topics are measured in a manner consistent with other federal surveys.
Another driver of the redesign – concern about response rates and costs – has remained the same across the decades. This passage describing the 1982-1996 NHIS could easily have been written today:
“… interviews averaged two hours. This imposed an unacceptable burden on NCHS staff, U.S. Bureau of the Census interviewers, the data collection budget, and, most importantly, on the NHIS respondents. Furthermore, the excessive length of NHIS interviews contributed to declines in both response rate and data quality. For all of these reasons, NCHS initiated a redesign of the NHIS questionnaire that was implemented in 1997.”
Redesign is an important part of the lifecycle of the NHIS, ensuring that the most relevant and highest quality information is collected and shared.
How Will the Content on the NHIS Change?
The content of the redesigned NHIS questionnaire will be more streamlined than the 1997-2017 NHIS. Duplicative questions will be eliminated, and there will be a reduced focus on the identification of rare health conditions and behaviors, which may result in fewer detailed follow-up questions to small segments of the population.
The key content areas for the redesigned NHIS are consistent with those on the 1997-2017 NHIS:
- Functioning and disability
- Health status and conditions
- Health insurance coverage
- Health care access and utilization
- Health risk behaviors
- Demographics
- Social and economic determinants of health
The changing nature of health research has led to newly-proposed content in several areas, including children's health, mental health, and social determinants of health.
How Will the Structure of the NHIS Change?
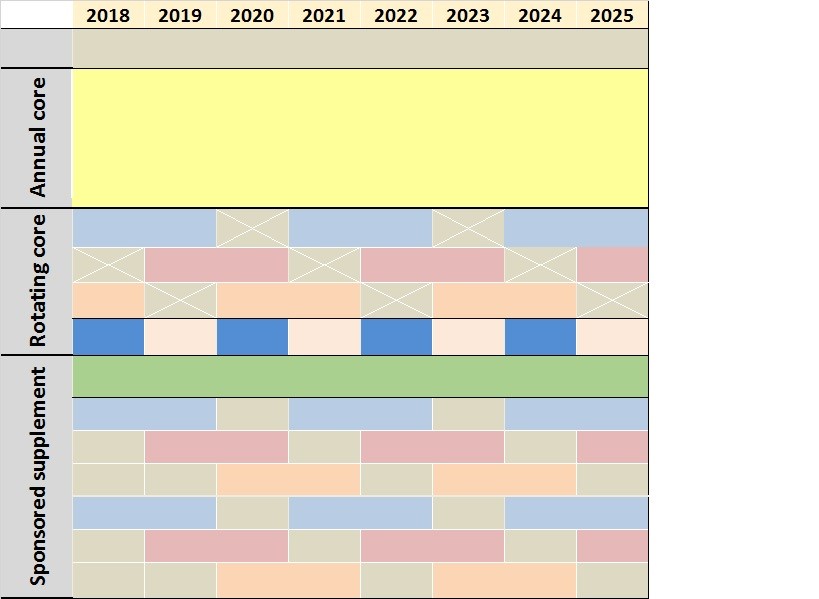
To maintain the breadth of content while reducing interview time, many key questions on the NHIS will be asked every year (“annual core”), with some questions only asked in some years (“rotating core”), as illustrated in Figure 1. Most of these rotating areas will overlap at least twice in the decade to provide researchers a wide selection of variables to study changes over time. Additional sponsored supplemental content may be funded by federal or health-related non-profit agencies. Depending on the sponsor’s needs, these questions may go on the NHIS for one or two years or with greater frequency. “Sustaining” sponsors may also commit to adding content annually.
For NHIS interviews in 2018 and beyond, NCHS proposes that one “sample adult” aged 18 years and over and one “sample child” aged 17 years and under (if any children live in the household) will be randomly selected from each household. Information about the sample child will be collected from a knowledgeable adult. This differs from the technique used in the 1997-2017 NHIS, which collected data about the family as a whole and about each member of the family before collecting detailed health data from a sample adult and about a sample child.
How is NCHS Getting Input from Users?
The NHIS has asked for feedback from the general public in four waves since October 2015. Expert opinion was also obtained in four key areas: children’s health, income, pain, and injury. Leaders in these fields from government, academia, private industry, and clinical practice contributed to discussions about priority setting for each topical area.
Staff at the NHIS greatly appreciate the time and careful thought that all of our data users and partners have contributed to this effort, and have read and discussed every comment that was received. From these discussions with experts, federal agencies, and the general public, a few common themes emerged. First, that NHIS should continue to emphasize areas that have traditionally been focal points of the survey. Second, that there were areas that needed an expansion of content to be of the most service to data users. Third, that some important health topics were better assessed by sources other than respondent self-report.
Continue to Emphasize
Data on many dimensions of health insurance, health care access and utilization, chronic conditions, and health behaviors have been focal areas for the survey and will still be collected in the redesigned NHIS. Feedback in these areas have helped to further refine how these topics will be addressed. The redesigned NHIS will continue to identify people with functional limitations and difficulties as well as collect data on contextual variables like family-level income.
Need to Expand
Some feedback emphasized the importance of family structure and family context, encouraging discussions with data users about which crucial content areas should be maintained even while moving away from the family interview. Content on mental health symptoms and treatment has been expanded in both the annual and rotating core in response to feedback. Expert opinion was very influential in updating the content on the sample child interview.
Choose the Best Source for Information
Experts and the public identified topics that are difficult to assess due to respondents’ limited knowledge or recall ability. Some topic areas (e.g., specialty areas or training of providers seen) have been dropped as a result. Other areas (e.g., food and beverage intake) were suggested in comments, but are already measured in more detail on existing nationally representative surveys.
More work remains to be done. For example, further development is needed to align questions on preventive services with national recommendations and to capture critical data on injuries. The collection of additional demographic information is being considered for all household members in addition to sample adults and sample children. All content areas and questions in this proposal remain subject to change and revision as comments are received.
How Can You Contribute?
Staff at the NHIS continue to welcome all comments on the proposed content and question text, how often the content is fielded, and ideas to reduce respondent burden and streamline the questionnaire. In addition, this is the first opportunity for providing feedback on draft questions. A public comment period is open through November 7, 2016. Please visit http://www.cdc.gov/nchs/nhis/2018_quest_redesign.htm for more information or provide comments through the Federal Register at regulations.gov (Docket ID: CDC-2016-0092).
Renee Gindi is a health survey statistician with the Division of Health Interview Statistics at the National Center for Health Statistics.
This blog post is sponsored by the Friends of NCHS.